
CCUIH Policy
What We Do
For inquiries, please contact policy@ccuih.org
Urban Indian Health Policy & Budget Monthly Updates
Click on any month to expand and read that report. Check back in each month to see what the CCUIH policy team has been up to!
Urban Indian Health Policy & Budget Update – February 2026
To download the full legislative report, click here.
Executive Snapshot
| Priority Issue | Timing | Why It Matters to UIOs | CCUIH Action |
| IHS Urban Indian Health Program Realignment | Comments due Feb 27, 2026 | May affect UIO oversight and funding structure. | Coordinating Urban comments and unified response. |
| Medi-Cal H.R.1 Implementation (AI/AN Definition) | State planning underway | Could impact AI/AN eligibility and coverage continuity. | Engaging DHCS and supporting UIO readiness. |
| Assembly Budget Hearing – H.R.1 & Workforce | Feb 23, 2026 | May shape California’s Medi-Cal and workforce response. | Reviewing proceedings and providing member analysis. |
| Senate Budget Hearing – Federal Impacts | Feb 26, 2026 | Addresses federal funding impacts to state health programs. | Monitoring and assessing UIO implications. |
| DHCS Tribal & Indian Health Program Meetings | Feb 23 & Feb 27, 2026 |
Affects Medi-Cal implementation and 1115 renewal. | Coordinating Urban priorities and sharing updates. |
| FY 2026 Labor–HHS Appropriations | Enacted Feb 3, 2026 |
Continues funding for key Native health programs. | Reviewing allocations and tracking implementation. |
| 340B Rebate Model RFI | Comments due Mar 19, 2026 | May affect UIO pharmacy reimbursement. | Analyzing impacts and evaluating comments. |
| CDC Public Health Grant Litigation | Ongoing (Feb 2026) |
Could disrupt public health funding in CA. |
Monitoring proceedings and potential impacts. |
Indian Health Service (IHS) Updates
- IHS Urban Indian Health Realignment / Consolidation Proposal (Jan 27, 2026): IHS issued a letter to Tribal Leaders and Urban Indian Organization Leaders describing a proposed realignment/consolidation of the Office of Urban Indian Health Programs and extended the comment period to February 27, 2026.
- Potential Impact to UIOs: Depending on the final approach, changes could affect program oversight, communication channels, and processes tied to UIO contracts and funding. CCUIH is monitoring and will share
member-facing coordination as needed. - CCUIH Action: In 2025, submitted written comment letters, developed member talking points, and provided verbal input during Urban Confer and consultation sessions. In 2026, continuing engagement by submitting
written comment guidance to IHS, developing template letters for UIOs, coordinating member input, and advancing unified Urban priorities through consultation and confer processes.
- Potential Impact to UIOs: Depending on the final approach, changes could affect program oversight, communication channels, and processes tied to UIO contracts and funding. CCUIH is monitoring and will share
- IHS Hiring Initiative (Jan 29, 2026): IHS issued a letter outlining a hiring initiative intended to improve staffing capacity across IHS.
- Potential Impact to UIOs: While the initiative focuses on IHS staffing, implementation may influence referral networks, collaboration with IHS partners, and federal operational capacity that interacts with urban Indian health programs.
- CCUIH Action: Will share updates with members and monitor for
operational impacts to UIO collaboration and referral systems.
- March 3–5, 2026: Annual California Tribal Consultation & Listening Session (Pala, CA); registration information circulated to Tribal and Urban leaders
- CCUIH Action: Submitted Urban Confer agenda items; preparing talking points and briefing materials for members; coordinating Urban
participation strategy; and convening the CCUIH Board Meeting in
conjunction with the session..
- CCUIH Action: Submitted Urban Confer agenda items; preparing talking points and briefing materials for members; coordinating Urban
California State Updates
- Legislative Deadlines: The California State Senate’s 2026 legislative deadlines calendar lists February 20, 2026 as the last day for bills to be introduced.
- CCUIH Action: Will review introduced legislation; identify measures with operational, funding, or policy implications for UIOs; provide member-facing impact analyses; and engage through comment letters or committee outreach as warranted.
- Assembly Budget Hearing (Feb 23, 2026): Assembly Budget Subcommittee No. 1 on Health held an informational hearing on California’s Response to H.R.1 (Part 1) and physician workforce development (Room 437).
- CCUIH Action: Will obtain and review hearing materials and testimony; document key takeaways affecting UIOs; share analysis with members; and engage committee staff as appropriate.
- Senate Budget Hearing (Feb 26, 2026): Senate Budget and Fiscal Review Subcommittee No. 3 (Health and Human Services) scheduled an informational hearing on “Federal Actions and their Impacts on State Programs and Funding Sources.”
- CCUIH Action: Will obtain and review hearing materials and testimony; document key takeaways affecting UIOs; share analysis with members; and engage committee staff as appropriate.
- DHCS Tribal and Indian Health Program Representatives Meeting (Feb 23, 2026): DHCS held a hybrid meeting (virtual and in-person, Sacramento) from 9:00 AM–4:00 PM PT. The CalAIM Section 1115 Demonstration Renewal discussion was scheduled from 2:00–3:15 PM PT.
- CCUIH Action: Policy staff in attendance; track statements and proposals relevant to Urban AI/AN communities; provide follow-up analysis to members; submit written comments or engage with committee staff as appropriate; and identify opportunities to ensure UIO inclusion in subsequent budget or policy proposals.
- DHCS Tribal and Designees of Indian Health Programs Quarterly Webinar (Feb 27, 2026): DHCS scheduled a virtual webinar from 2:00–3:00 PM PT on proposed changes to the Medi-Cal Program, including updates related to the CalAIM Section 1115 Demonstration Renewal.
- CCUIH Action: Policy staff in attendance; track statements and proposals relevant to Urban AI/AN communities; provide follow-up analysis to members; submit written comments or engage with committee staff as appropriate; and identify opportunities to ensure UIO inclusion in subsequent budget or policy proposals.
- DHCS H.R.1 Implementation Planning (Jan 29, 2026): DHCS published a statewide implementation plan outlining effective dates and operational considerations for H.R.1 changes to Medi-Cal.
- Broad Definition of AI/AN (for eligibility/reporting purposes) An individual qualifies as American Indian/Alaska Native if they:
- Self-identify as American Indian or Alaska Native, either alone OR in combination with any other race or ethnicity, AND
- Are identified or registered as American Indian by a Tribal Health Program (THP) for purposes of reporting or service documentation.
- CCUIH Action: Reviewing DHCS implementation guidance to ensure the broadest permissible definition of AI/AN is applied in practice; engaging DHCS to clarify eligibility and exemption standards; coordinating with UIOs to assess operational impacts; and developing patient-facing education and technical support to ensure Urban AI/AN individuals understand their eligibility protections and maintain Medi-Cal coverage.
- Broad Definition of AI/AN (for eligibility/reporting purposes) An individual qualifies as American Indian/Alaska Native if they:
Federal Updates
- FY 2026 Labor-HHS Appropriations Enacted (Feb 3, 2026): Congress passed and the President signed the FY 2026 Labor, Health and Human Services, and Related Agencies appropriations bill as part of the Consolidated Appropriations Act, 2026. Reported Native health-related items include $200 million for the Special Diabetes Program for Indians (SDPI), $27 million for Good Health and Wellness in Indian Country, $9 million for the Improving Native American Cancer Outcomes program, approximately $25.67 million for Tribal Behavioral Health Grants (Native Connections), and report language establishing a Tribal set-aside within the National Health Service Corps that includes support for Urban Indian Health Programs.
- CCUIH Action: Analyzing funding allocations and report language; disseminating summaries to members; monitoring implementation timelines; and identifying funding or partnership opportunities relevant to UIO operations.
- HRSA 340B Rebate Model RFI (Feb 13, 2026; comments due Mar 19, 2026): HRSA released a Request for Information (RFI) on a 340B Rebate Model Pilot Program, restarting notice-and-comment work after the prior model pause.
- CCUIH Action: Analyzing potential impacts to UIO 340B operations; coordinating with partners; and evaluating submission of written comments prior to the March 19 deadline.
- CDC Public Health Grant Terminations (Feb 2026): HHS/CDC notified Congress of its intent to terminate roughly $600M in CDC public health grants to California, Colorado, Illinois, and Minnesota. States filed suit challenging the action and a federal judge granted a temporary restraining order blocking the cuts pending further litigation.
- CCUIH Action: Tracking court proceedings and state response; evaluating potential effects on public health infrastructure that interacts with UIOs; and communicating relevant updates to members.
Shaping AI/AN Health Policy: Where We’ve Been
The CCUIH policy team has been actively engaged in key spaces shaping AI/AN health policy, advocacy, and strategy.
- MMIP Summit – Engaging in statewide MMIP prevention, safety, and cross-system coordination efforts.
- NCAI – Tracking federal Indian health policy and national advocacy priorities.
- DUIA Urban Program Executive Directors – Coordinating with UIO leadership on funding, implementation, and system alignment.
- CalHHS 988 – Crisis Policy Advisory Group – Providing input to ensure culturally responsive 988 crisis implementation for AI/AN communities.
- THCP Community Advisory Board – Advising on Traditional Health Care Practices implementation and community-informed guidance.
- Indian Health Collaborative – Aligning partners to strengthen the Indian Health delivery system across Tribal and Urban settings.
- H.R. 1 Implementation – DHCS – Monitoring Medi-Cal exemption and AI/AN definition implementation impacts on UIOs.
- IHS CAO Planning Studies Workgroup – Engaging in PRCDA planning and data transparency discussions.
- CPEHN Statewide Health Equity – Collaborating on statewide health equity advocacy and budget priorities.
- Community Health Worker (CHWs) Policy Group – Advancing CHW policy, reimbursement, and workforce sustainability efforts.
- NCUIH Policy Workgroup – Tracking federal policy developments affecting UIOs. (Meeting Monthly with NCUIH one-on-one focused on CA updates).
- CPCA All Member & Board Meetings – Representing Urban Indian priorities in statewide health center advocacy.
- CDPH Tribal Health Equity Advisory Group (THEAG) – Informing CDPH health equity strategies from an AI/AN perspective.
- Meetings with UIOs on TH/NH & Counties – Supporting UIOs in county coordination and TH/NH implementation efforts.
Governor’s 2026–27 January Budget Snapshot for Urban Indian Organizations
To download the full legislative report, click here.
Executive Summary
The Governor’s January 2026–27 Budget proposal spans more than 300 pages and initiates the state’s annual budget process. This document provides a high-level synthesis of the portions most relevant to Urban Indian Organizations (UIOs), recognizing that the January proposal reflects preliminary assumptions rather than final funding levels or implementation decisions. Overall, the proposal largely continues existing investments across Medi-Cal, behavioral health, workforce, and education systems; for UIOs, the most consequential impacts will be shaped less by topline funding amounts and more by how programs are implemented through subsequent legislative action, state guidance, and county-level administration. This summary is intended to support situational awareness and planning by highlighting structural dynamics that may affect access to care, reimbursement stability, workforce capacity, and service demand for urban American Indian and Alaska Native communities, and does not represent final budget outcomes or recommend specific policy actions.
4 Key Areas With Potential Impact to UIOs
- Medi-Cal Cost Pressures = Downstream Risk for UIOs
The budget identifies $1.1 billion in additional Medi-Cal costs driven by recent federal policy changes (H.R. 1 of 2025), with no major new state backfill proposed. A significant share of Medi-Cal financing relies on provider taxes and fees that are subject to federal rules and timing constraints; changes or delays in these funding sources can create short-term uncertainty for reimbursement stability across the safety-net system. Ongoing eligibility and administrative changes within Medi-Cal may also contribute to coverage churn, disrupting continuity of care and increasing administrative burden for clinics serving high-need and mixed-status populations.
Why this matters for UIOs
UIOs serve a disproportionately Medi-Cal–enrolled patient population. As a result, shifts in Medi-Cal financing or administration can have immediate operational impacts, including:
- Increased patient navigation and eligibility support needs
- Cash-flow uncertainty tied to reimbursement timing
- Higher uncompensated care pressures
Together, these dynamics underscore the importance of reimbursement stability, timely program implementation, and administrative continuity for providers serving urban American Indian and Alaska Native communities.
- Behavioral Health Investments
The state cites more than $10 billion invested across the behavioral health continuum in recent years and proposes to continue implementation of existing initiatives. However, the proposed budget does not add substantial new ongoing state funding, meaning service availability and access will continue to depend largely on local implementation decisions, administrative capacity, and provider inclusion.
Potential Implications for Urban Indian Organizations
Opportunities for Urban Indian Organizations are most likely to materialize when UIOs are explicitly included in program design and contracting by counties and state agencies. In practice, behavioral health funding frequently:
- Flows through county-administered systems
- Does not consistently include Urban Indian providers as eligible contractors ● Fails to reach American Indian and Alaska Native patients in urban settings
These dynamics are particularly relevant for:
- 1115 waiver implementation, including Traditional Healers, Community Health Workers, and behavioral health services
- County pass-through contracting and reimbursement timelines
In short, funding may be available, but access for urban AI/AN patients and providers is shaped by implementation choices rather than funding levels alone.
- Workforce & Labor Investments
The proposed budget continues statewide workforce and labor investments but does not include targeted adjustments for high-cost urban healthcare markets or specific strategies addressing parity for Tribal Health Programs and Urban Indian Organizations.
Implications for Urban Indian Organizations
Absent targeted workforce strategies, Urban Indian Organizations continue to face structural challenges related to:
- Recruitment and retention in competitive urban labor markets
- Wage competition with hospital systems and large health networks
- Sustaining culturally grounded workforce models that require additional training and support
No geographic cost adjustment or UIO-specific workforce approach is identified in the proposal, which may limit the impact of broader workforce investments for providers serving urban American Indian and Alaska Native communities.
- Education & Community School Investments: Indirect Touchpoints
The budget includes large ongoing investments in education-related systems, including: ● Community schools
- School-based behavioral health
- Early childhood education and family support programs
Why this matters for UIOs (Indirectly)
UIOs that partner with Local Education Agencies (LEAs) or serve families connected to these systems may experience:
- Increased referral volume for behavioral health and supportive services ● Greater demand for care coordination and family-centered services
However, UIOs are not consistently identified as eligible lead entities within these education-focused initiatives, which may limit direct access to funding despite increased service demand.
|
What This Budget Signals Strategically for CCUIH and UIOs ● Program stability is a central consideration. With continued cost pressures and implementation-dependent funding, maintaining Medi-Cal access, reimbursement continuity, and existing financing pathways remains critical for providers serving urban AI/AN communities. ● Implementation decisions will shape real-world impact. The effects of the proposed budget will be determined largely by how state agencies and counties operationalize programs, underscoring the importance of monitoring implementation and provider inclusion. ● Data visibility will continue to influence future decisions. Without consistent identification of Urban American Indian and Alaska Native populations and Urban Indian Organizations in data collection and reporting, service utilization and community needs may remain underrepresented in future budget development. |
Budget Timeline and What to Expect Next
January–February: Governor’s Budget Release and Initial Review
- The Governor’s January Budget proposal establishes baseline assumptions for the upcoming fiscal year.
- State agencies begin internal planning based on the proposal, but no final decisions are made at this stage.
- Budget documents are reviewed by the Legislature and stakeholders to identify key issues and areas requiring clarification.
- What this means for UIOs:
This is an orientation phase. Program details, funding levels, and implementation approaches are still preliminary.
- What this means for UIOs:
February–April: Legislative Budget Hearings and Analysis
- Legislative budget subcommittees hold hearings on major program areas, including Medi-Cal, behavioral health, workforce, and education.
- Assumptions and proposals may be questioned, adjusted, or held open for revision. ● State departments may begin informal conversations about implementation scenarios.
- What this means for UIOs:
This period shapes how programs are understood and framed, but most operational details remain undecided.
- What this means for UIOs:
May: Governor’s May Revision
- The Governor releases the May Revision, updating the budget based on revised revenue estimates and policy adjustments.
- This is often when significant changes occur to Medi-Cal assumptions, program funding levels, and timelines.
- What this means for UIOs:
This is a key checkpoint for identifying material changes that could affect reimbursement, eligibility, or service delivery.
- What this means for UIOs:
June: Budget Adoption
- The Legislature passes a budget by June 15.
- The adopted budget reflects negotiated funding levels but often leaves policy and implementation details unresolved.
- What this means for UIOs:
Funding amounts may be finalized, but how programs operate is frequently determined later.
- What this means for UIOs:
Summer–Fall: Trailer Bills and Implementation
- Policy “trailer bills” are adopted to establish program rules, eligibility, provider participation, and administrative processes.
- State agencies issue guidance, and counties begin implementation planning.
- What this means for UIOs:
This phase determines real-world impact — including provider inclusion, contracting pathways, and reimbursement timing.
- What this means for UIOs:
How UIOs Can Use This Information
This summary is intended to support awareness and planning, not to require action. UIOs may consider:
- Monitoring updates from CCUIH related to the May Revision, trailer bills, and agency guidance
- Identifying potential operational impacts, such as changes to Medi-Cal enrollment patterns, reimbursement timing, or service demand
- Preparing internal questions related to county implementation, contracting, or eligibility as details become clearer
- Sharing relevant operational data when requested to support accurate representation of urban AI/AN service utilization
CCUIH will continue to track budget developments and implementation milestones and provide updates as information relevant to Urban Indian Organizations becomes available.
2025 Year in Review & 2026 Look Ahead
Click here to download the full Legislative Report!
2025 was a year of significant operational and policy shifts for Urban Indian Organizations. Federal oversight increased, state reforms were delayed, and the federal shutdown disrupted funding and timelines. Behavioral health needs rose, Medi-Cal navigation demands grew, and UIOs continued supporting communities through MMIP-related needs and increasing youth behavioral health concerns. Workforce pressures and public health demands also persisted.
Looking ahead to 2026, UIOs will implement new privacy and data requirements and prepare for the return of major two-year bills early in the legislative session. Federal appropriations, grant timelines, and Medicaid policy proposals will continue to shape stability. UIOs enter this new year focused on continuity, preparation, and maintaining community-centered care amid ongoing system transition.
2025 YEAR IN REVIEW
MEDICAID & MEDI-CAL: Navigating a Shifting Landscape
Medi-Cal and Medicaid were highly dynamic in 2025. UIOs supported patients through coverage interruptions, administrative updates, and benefit planning.
- The federal shutdown delayed some grants, payments, and agency communications; IHS clinical operations continued due to advance appropriations.
- Federal Medicaid proposals created additional monitoring needs to ensure AI/AN protections remained intact.
- Medi-Cal redeterminations increased UIO administrative work on reinstatements and continuity of care.
- Several Medi-Cal bills were carried into 2026.
- TH–NH services began early Medi-Cal implementation, with UIOs and DMC-ODS counties working through reimbursement and documentation steps under the waiver through December 31, 2026
Bottom Line: Coverage and administrative changes increased navigation needs, and UIOs remained the main support for helping patients maintain Medi-Cal access.
BEHAVIORAL HEALTH: Rising Needs in a Transition Year
Behavioral health needs continued to increase for AI/AN communities, especially youth and families experiencing trauma and chronic stress.
- UIOs reported increased behavioral health demand, particularly for youth and families navigating trauma, stress, and crisis support needs.
- While new behavioral health funding was introduced statewide, no new funding streams were created specifically for UIOs or the I/T/U system.
- CYBHI advanced statewide, yet its school-centered design left gaps for youth receiving care in community settings such as UIO clinics.
- Documentation modernization required workflow adjustments.
-
The statewide behavioral health system transformation under BHSA shifts reforms from individual bills to a broad system overhaul effective July 1, 2026; counties are preparing integrated plans under the new framework.
-
Federal shutdown delays affected HRSA and SAMHSA grants.
-
Federal proposals and litigation affecting Medicaid/CHIP gender-affirming care required monitoring.
Bottom Line: Behavioral health needs grew while system updates were delayed, requiring UIOs to meet rising demand within existing resources.
MMIP: Ongoing Impacts on Health and Safety
MMIP continued to shape UIO work in crisis response, behavioral health, and family support.
- UIOs supported families through crisis navigation and follow-up care.
- Coordination challenges persisted across jurisdictions.
- MMIP bills stalled in 2025, with all major proposals continuing as two-year bills for action in 2026.
- Data access gaps remained across agencies.
Bottom Line: MMIP remains a major health and safety concern, and UIOs provide critical support without dedicated funding streams.
PUBLIC HEALTH & PREVENTION
Demand increased for prevention, chronic disease care, STI response, and MCH services.
- Increased volumes in MCH, chronic disease, and prevention programs.
- Federal shutdown delayed prevention grant timelines.
- Uncertainty about Marketplace subsidies beyond 2025 may cause more people to cycle in and out of coverage.
- Several reproductive and oral health laws take effect January 1, 2026.
Bottom Line: Public health needs grew in 2025 while funding stayed flat.
WORKFORCE
Workforce shortages remained a core challenge for UIOs in 2025.
- Shortages persisted across SUD, primary care, MCH, and prevention roles.
- Workforce bills moved to 2026.
- Specialty care wait times increased across systems.
Bottom Line: Workforce limitations continued to affect service access and program growth.
DATA, REPORTING & PRIVACY
UIOs experienced a growing set of state and federal data requirements.
- SB 1016 Indigenous category planning began.
- New state privacy and health-data laws (including AB 45 and SB 278) taking effect January 1, 2026 will require new workflows and consent processes.
- Federal oversight increased under new directives.
- IHS/HHS modernization created uncertainty about Urban data pathways.
Bottom Line: New state and federal data requirements require planning and system updates in early 2026.
340B & PHARMACY
Major changes to 340B will affect UIO pharmacy operations in 2026.
- A federal 340B rebate model pilot begins January 1, 2026 for selected drugs and participating entities.
- Certain drugs must be purchased at WAC up front.
- Rebates will come later, requiring new tracking processes.
- Contract pharmacy arrangements may need adjustments.
Bottom Line: The 340B rebate model will require operational and cash flow adjustments.
FEDERAL LANDSCAPE
Federal policy shifts in 2025 shaped funding, timelines, and oversight.
- Executive Orders increased oversight and documentation requirements.
- HHS restructuring created uncertainty around modernization timelines and Urban Confer. This is paused due to pending legal action.
- Shutdown delayed grants, payments, and technical assistance.
- SDPI remained on temporary authorization.
- PRWORA-related discussions required ongoing monitoring.
- Federal Medicaid proposals — including eligibility tightening, gender-affirming care restrictions, and work-requirement discussions — required monitoring to ensure AI/AN protections remained intact.
Bottom Line: Federal activity introduced delays, oversight requirements, and shifting priorities that UIOs had to plan around.
2026 Look AheadKey Dates● January 1, 2026: Most 2025 chaptered laws take effect ● January 1, 2026: 340B rebate model begins ● January 31, 2026: Two-year bill deadline ● Federal appropriations remain unresolved entering 2026 Operational Priorities● TH–NH documentation and reimbursement workflows ● Implementation of 2026 privacy and data laws ● Adjustments for 340B rebate model ● Ongoing Medi-Cal redeterminations ● Rising Behavioral health needs linked to CARE Court and FSP updates
|
October End-of-Session
The 2025 California Legislative Session adjourned on September 13, and the Governor’s October 13 deadline to sign or veto bills has passed, finalizing the state’s legislative actions for the year. Several key health and public safety bills were signed, while many others moved to the inactive file, becoming two-year bills for 2026. Federally, the government shutdown that began on October 1 remains unresolved, with Congress still in recess, delaying appropriations and impacting grant processing and operational stability for UIOs. A special election in early November adds further uncertainty as state and federal budget debates evolve.
August 2025
August brought critical developments for Urban Indian Organizations (UIOs) at both the federal and state levels. Federally, we are deeply concerned with HHS’ reinterpretation of PRWORA, which expands verification requirements across benefit programs and creates new administrative and access risks for UIOs. FY 2026 appropriations remain unsettled, with the House proposing a $15M increase for Urban Indian Health and the Senate holding flat, while implementation of H.R. 1 (“One Big Beautiful Bill”) will begin in January 2026, reshaping Medicaid through cost-sharing, asset tests, and work rules—though AI/AN exemptions remain in place. Risks also persist around SAMHSA funding and new federal grant restrictions tied to equity language. At the state level, several Medi-Cal State Plan Amendments were noticed in August with September comment deadlines, and key bills on telehealth, community health workers, perinatal care, and patient privacy are advancing, while AB 1113 (restricting FQHC spending) became a two-year bill. Over 650 measures faced suspense hearings at the end of August, and SEIU-UHW has filed a 2026 ballot initiative that would impose new financial mandates on community health centers, raising significant concerns for UIO operations.
June 2025
May 2025
CCUIH 2025–26 MAY REVISION BUDGET POLICY ANALYSIS
Impacts on Urban Indian Organizations and AI/AN Communities
BUDGET LANDSCAPE :
The May Revision to the Governor’s 2025–26 Budget reflects a projected $12 billion shortfall, with significant reliance on deferrals, program delays, and spending reductions. While General Fund spending in Health and Human Services increases on paper, this section begins the detailed analysis of each budget area. It provides the foundation of the document by addressing the most direct and significant implications for Urban Indian Organizations (UIOs), particularly in Medi-Cal and public health policy. While the total Health and Human Services budget increases on paper, this growth is driven by rising Medi-Cal caseloads and federally mandated costs. For Urban Indian Organizations (UIOs), the budget presents serious structural risks, including care disruptions, uncompensated care burdens, and defunding of culturally grounded care models. The May Revision offers few, if any, targeted protections for American Indian and Alaska Native (AI/AN) communities in urban areas.
April 2025
All eyes are on May 14, when the Governor’s May Revision will be released—expected to outline a two-year spending plan with deep cuts across health and human services. CCUIH is monitoring closely for impacts to Urban Indian health, especially in behavioral health, workforce, and prevention. At the federal level, IHS announced it will maintain competitive behavioral health grant funding through FY27, continued its PATH EHR rollout, and included UIOs in revenue cycle planning. Meanwhile, the Trump administration’s upcoming budget proposal is expected to target Medicaid, IHS, and non-defense discretionary programs. In April, CCUIH testified on AB 1113, tracked 74 active state bills, and held nine congressional meetings during the NCUIH Annual Conference to defend UIO funding and share patient impact stories. The policy team also advanced coalition efforts with CPCA, CPEHN, DHCS, Cal Wellness, and others to shape state and federal policy for AI/AN health equity.
March 2025
The March 2025 Legislative Report highlights CCUIH’s advocacy at both the federal and state levels to ensure Urban Indian Organizations (UIOs) are prioritized in key policy decisions. At the federal level, CCUIH participated in the California Area IHS Urban Confer, emphasizing IHS accountability, data transparency, and financial stability for UIOs. As federal budget cuts loom, CCUIH is ramping up advocacy to protect UIO funding following the recent stopgap extension. The report also addresses potential IHS lease terminations and the urgent need for continued support. On the state side, CCUIH is advancing legislation on healthcare expansion, telehealth, and workforce development, with several priority bills moving forward. Additionally, DHCS released the long-awaited BHIN on reimbursement for Traditional Healers and Natural Helpers under the 1115 waiver—an important milestone for culturally responsive care. CCUIH will host an informational session for UIOs on March 31 to support implementation.
February 2025
The year has started with major challenges for Urban Indian health, from funding threats to policy changes that could impact care. CCUIH is actively engaged in advocacy, tracking key legislation, and preparing for critical discussions at the February 24 budget hearing. Now is the time for action—your voice and engagement are crucial to protecting Urban Indian health services.
January 2025
Legislative Developments:
Multiple bills we are tracking in the California State Assembly have been accepted and are currently being assigned to committees. (Expect a list of bills we are tracking coming your way in February). If there are any bills you are particularly interested in, please let us know.
Policy Updates:
1115 Waiver: The Department of Health Care Services (DHCS) guidance and opt-in guidance were submitted.
Upcoming Meeting: DHCS Tribal Health/Native Health (TH/NH), Tribes, and Indian Health Program Representatives Meeting is scheduled for Monday, February 3rd, 1-3 PM.
2024 Updates
Pocket-Sized Policy
View and download any graphic by clicking on it!
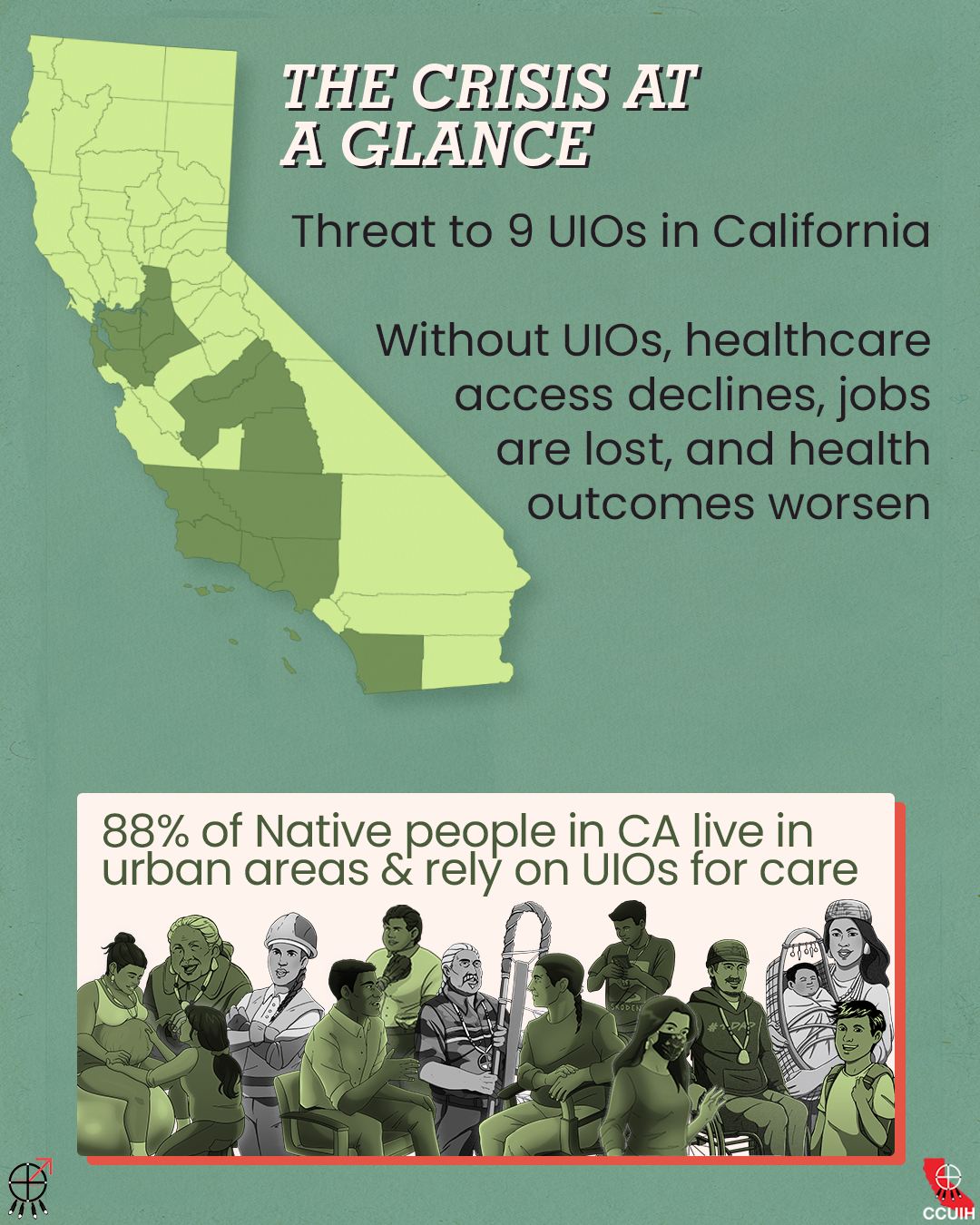
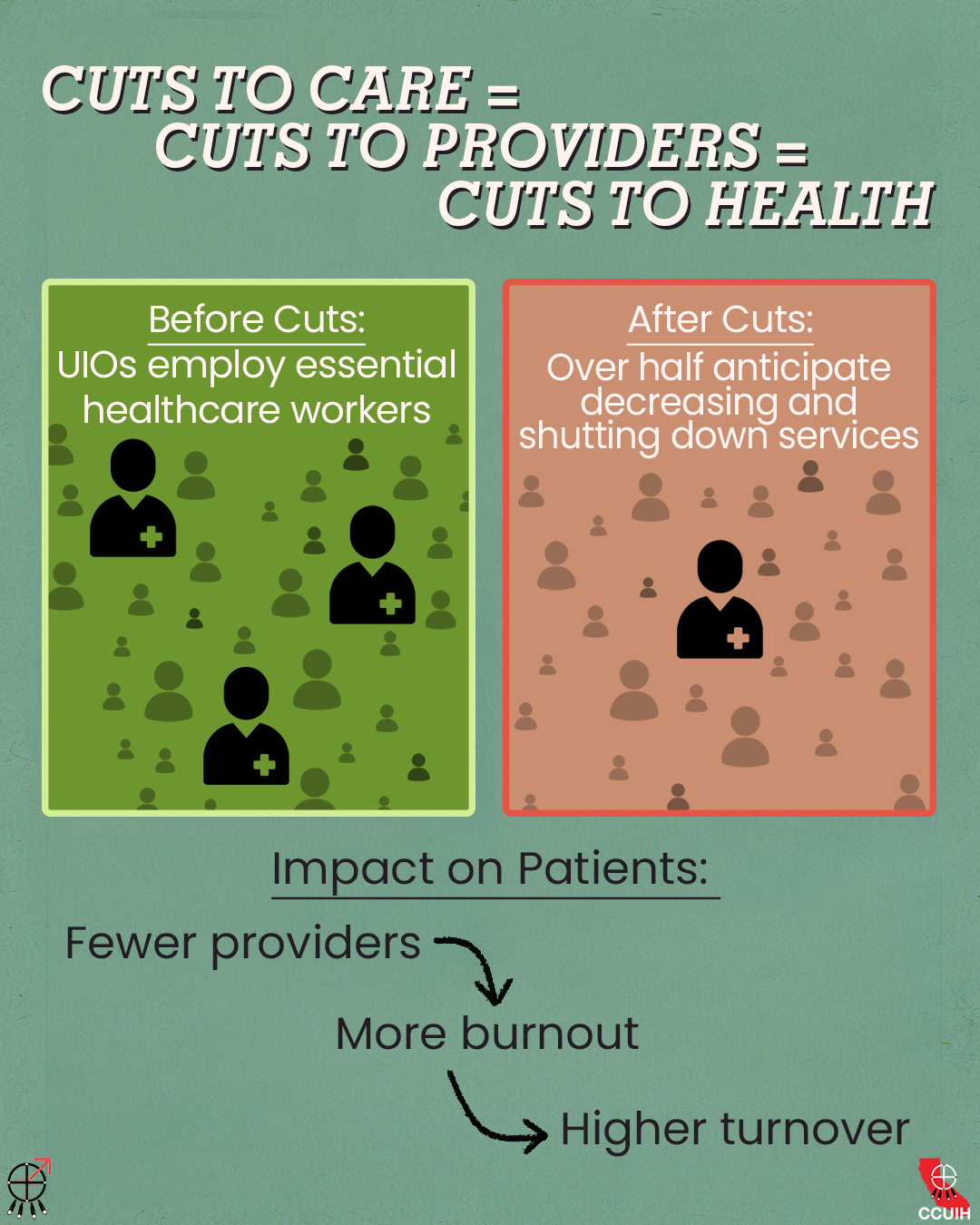
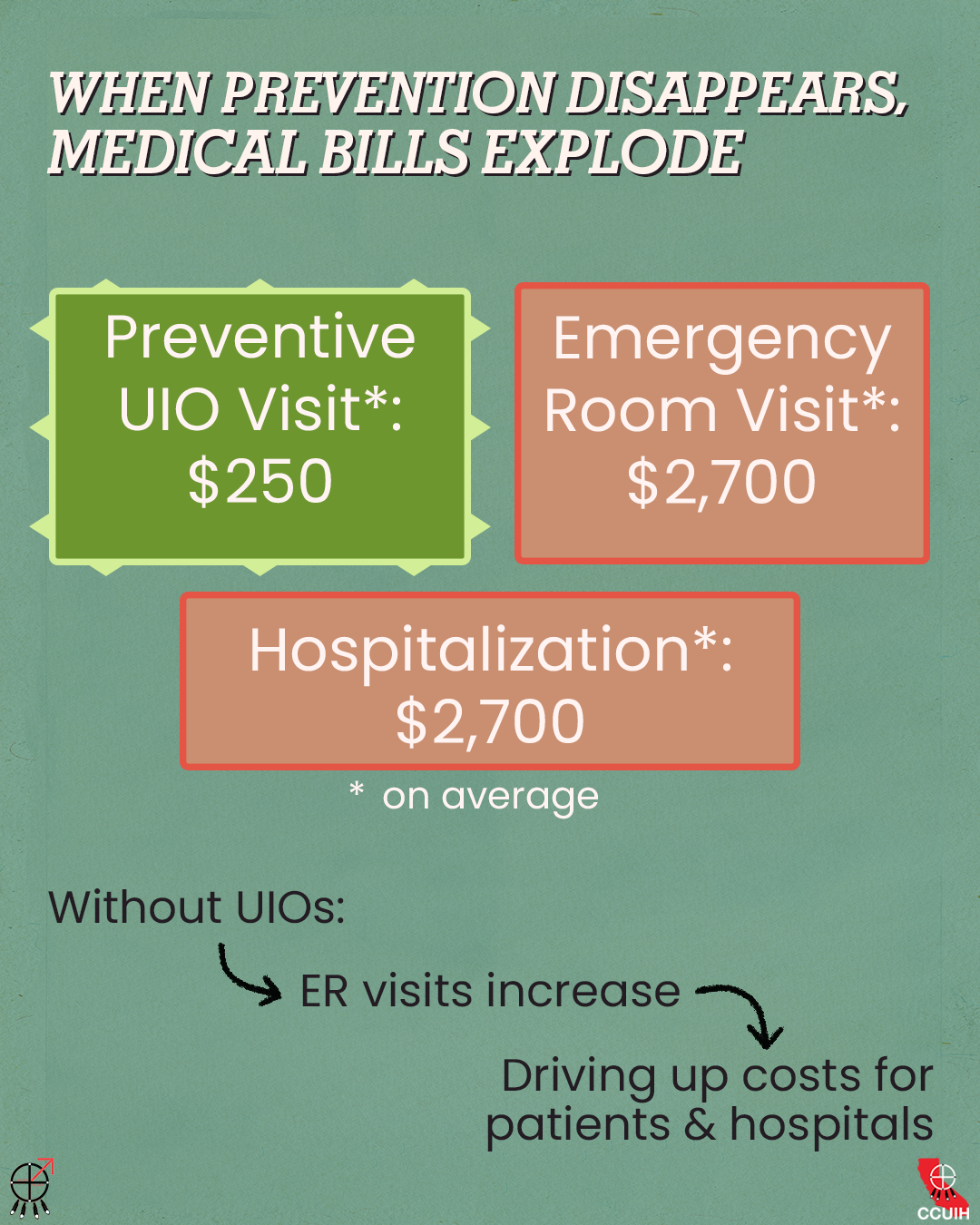
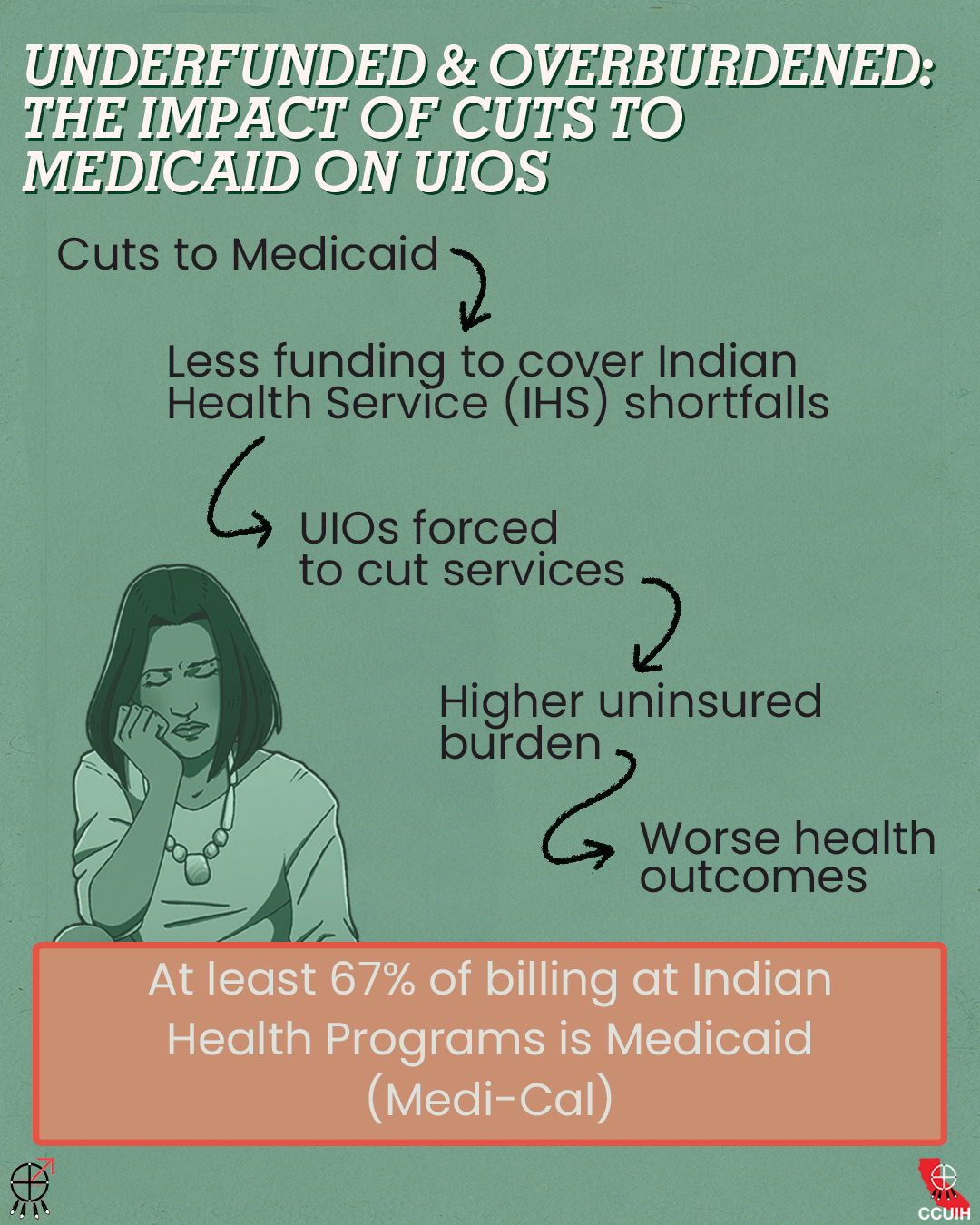
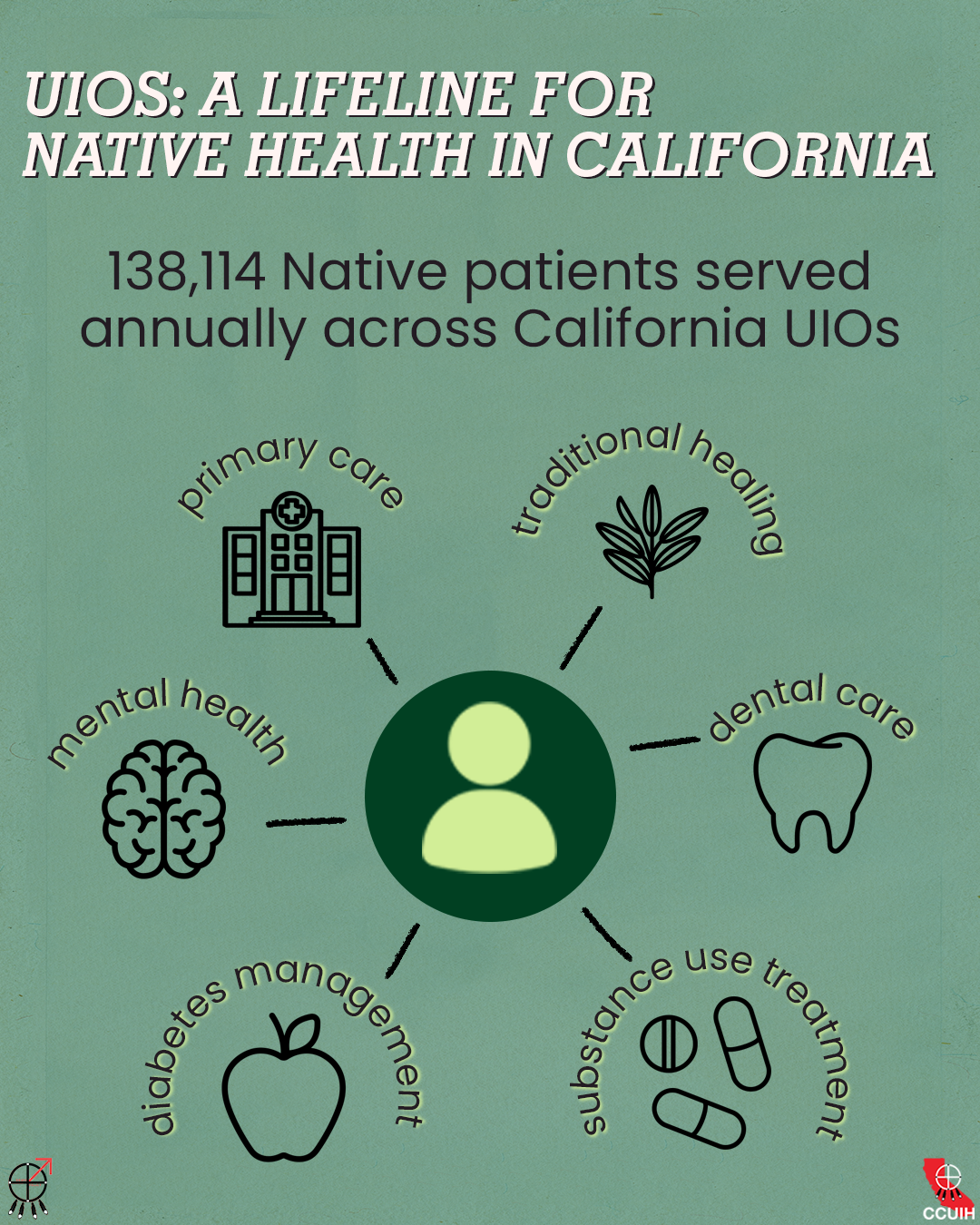
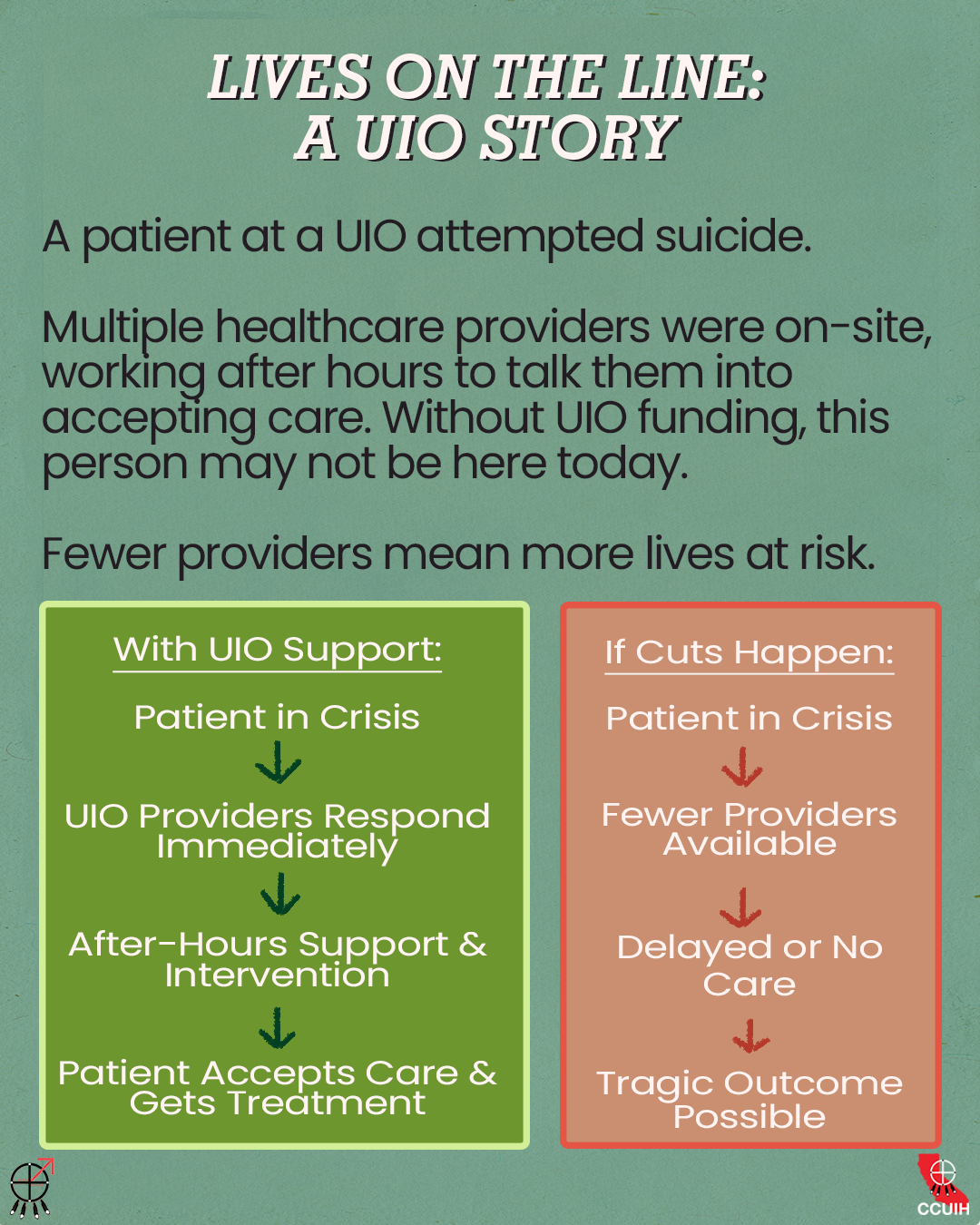
The True Cost of Medicaid Cuts on Urban Indian Health in California:
How Reductions in Medicaid Funding Harm Urban Indian Organizations (UIOs) and the Communties they Serve
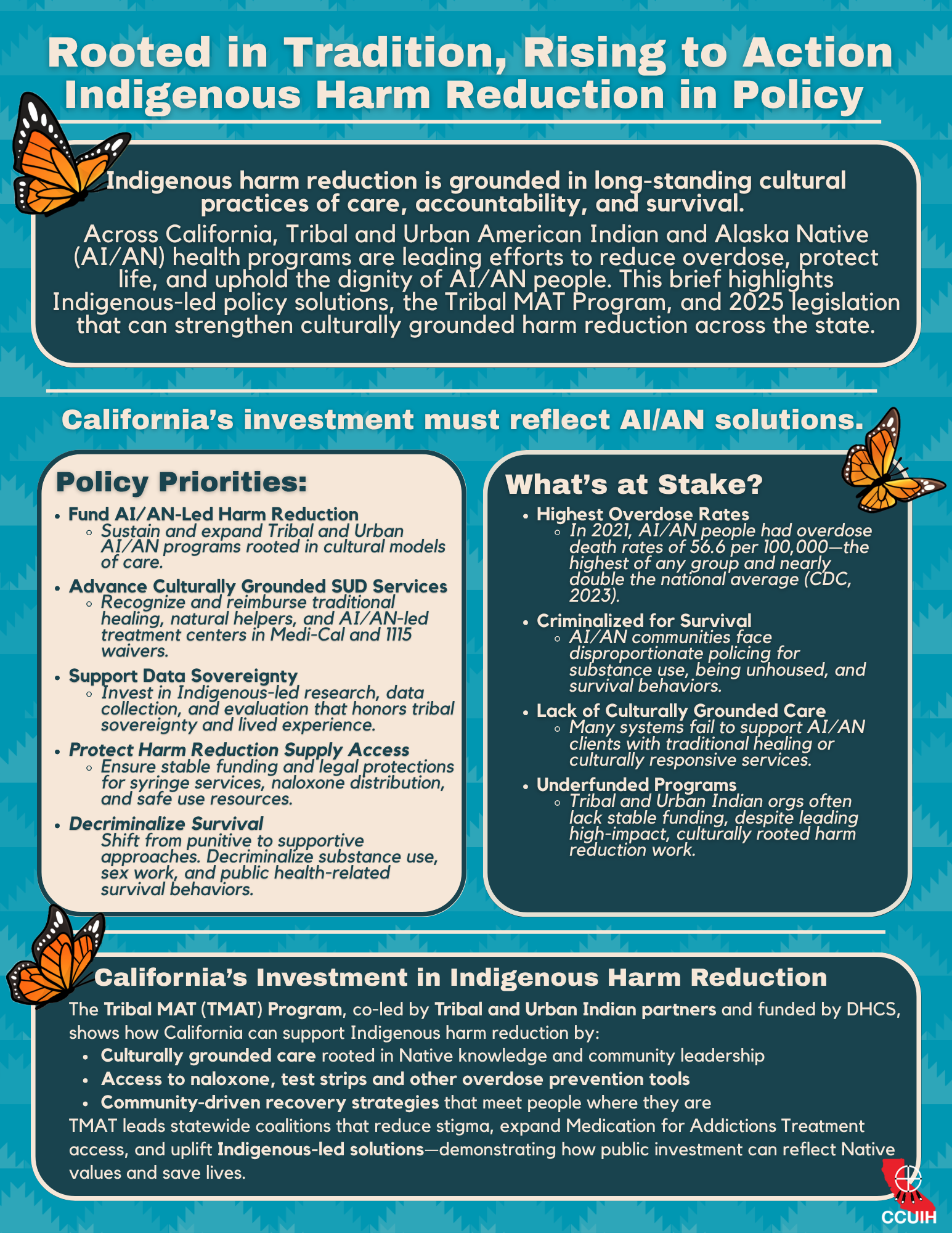
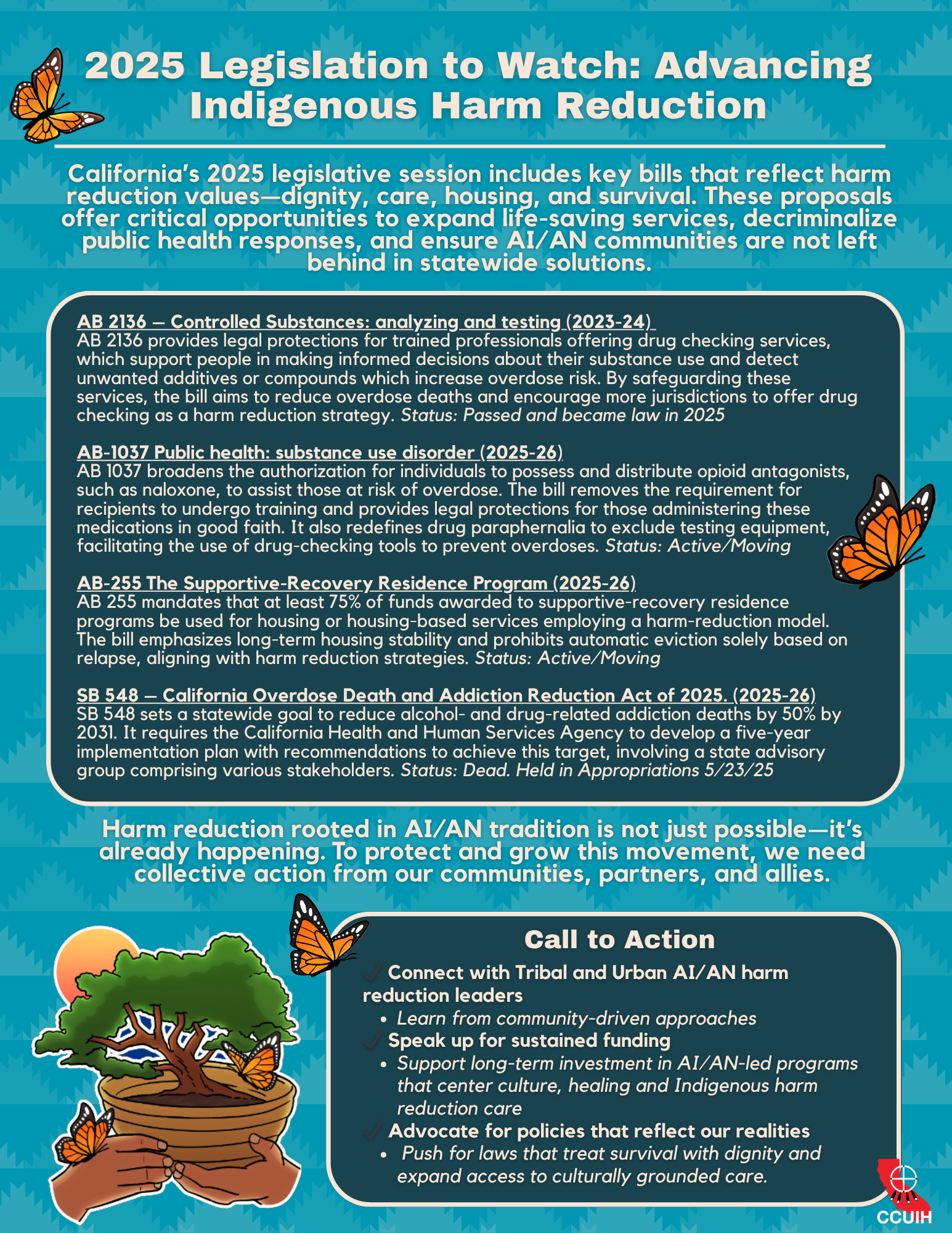
Rooted in Tradition, Rising to Action:
Indigenous Harm Reduction in Policy
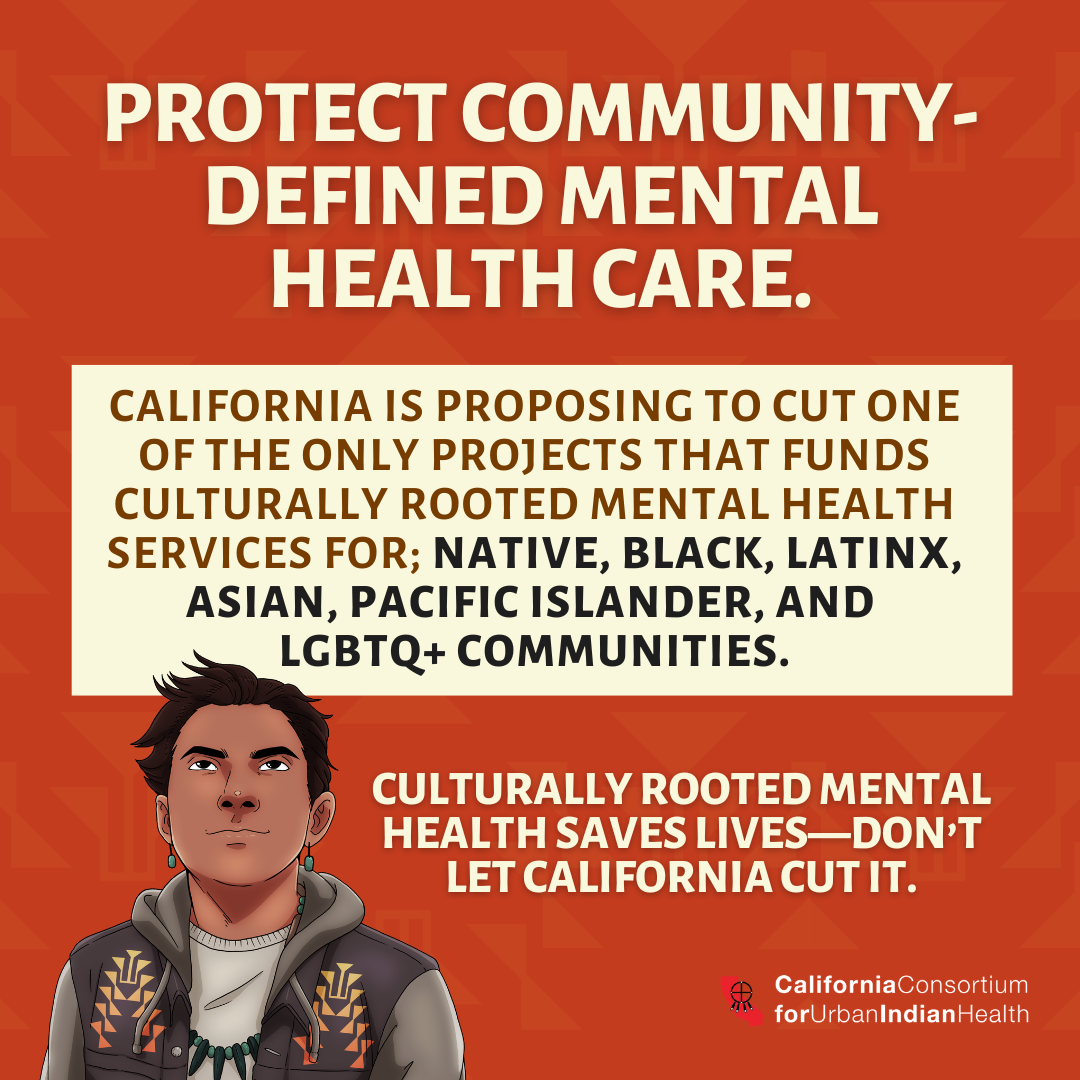
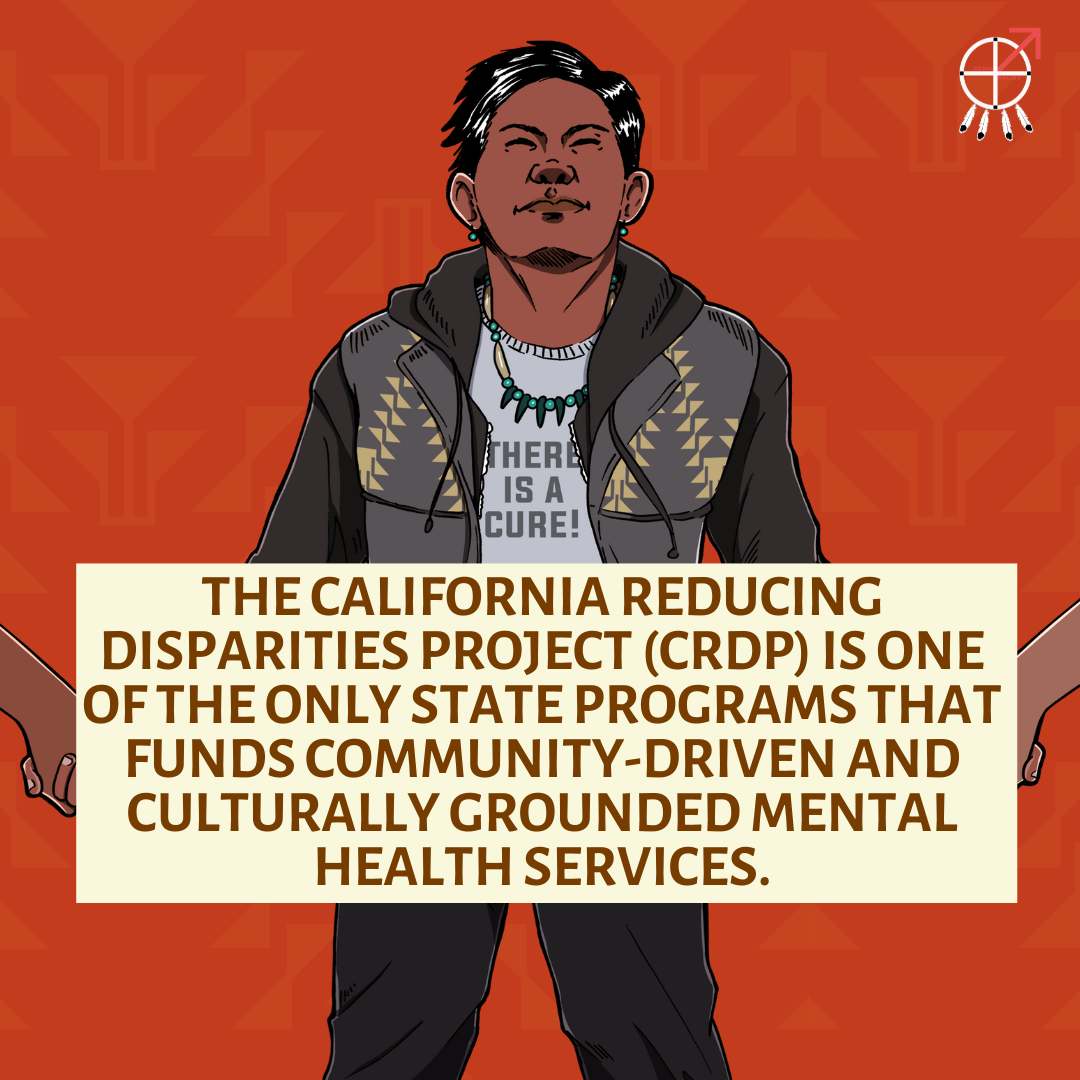
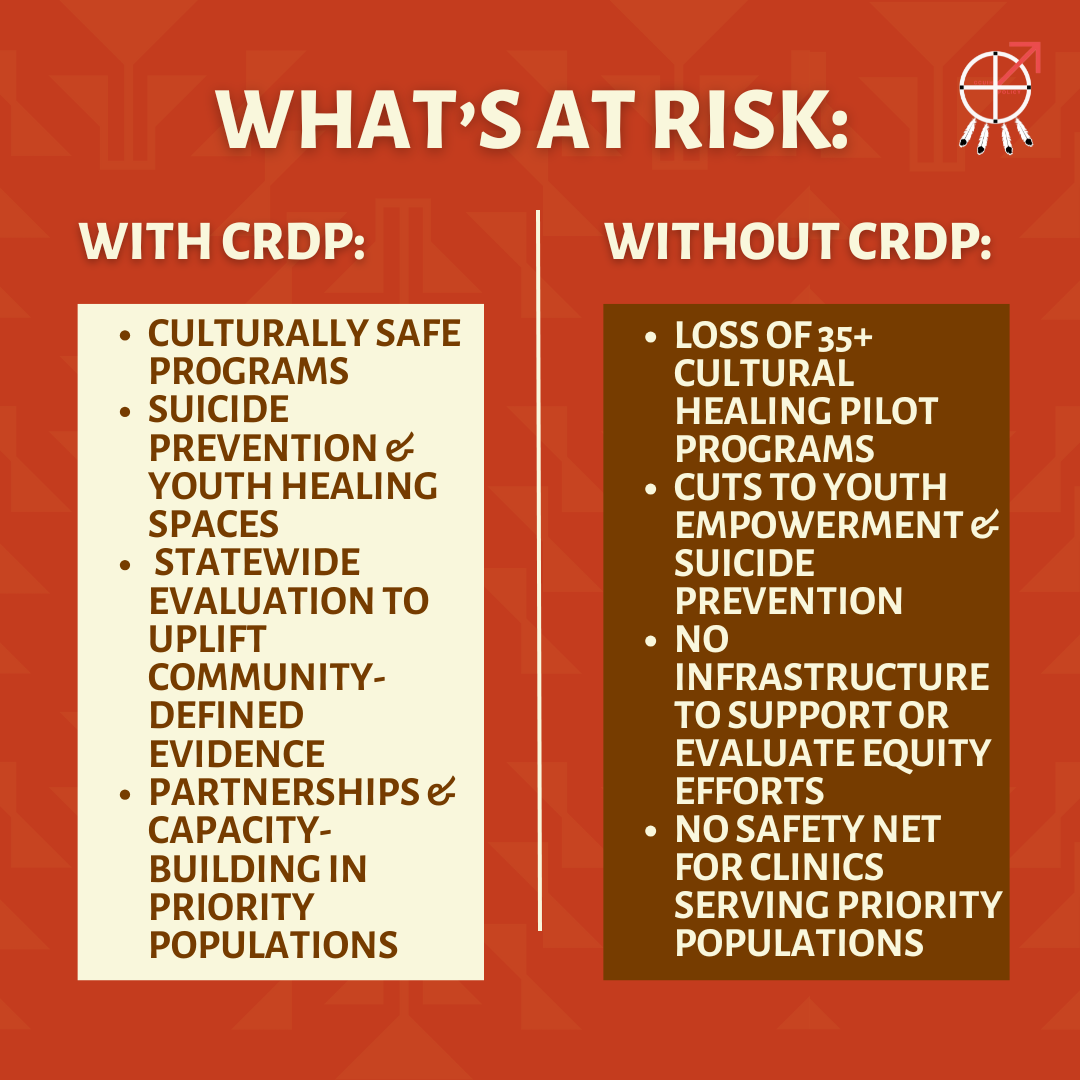
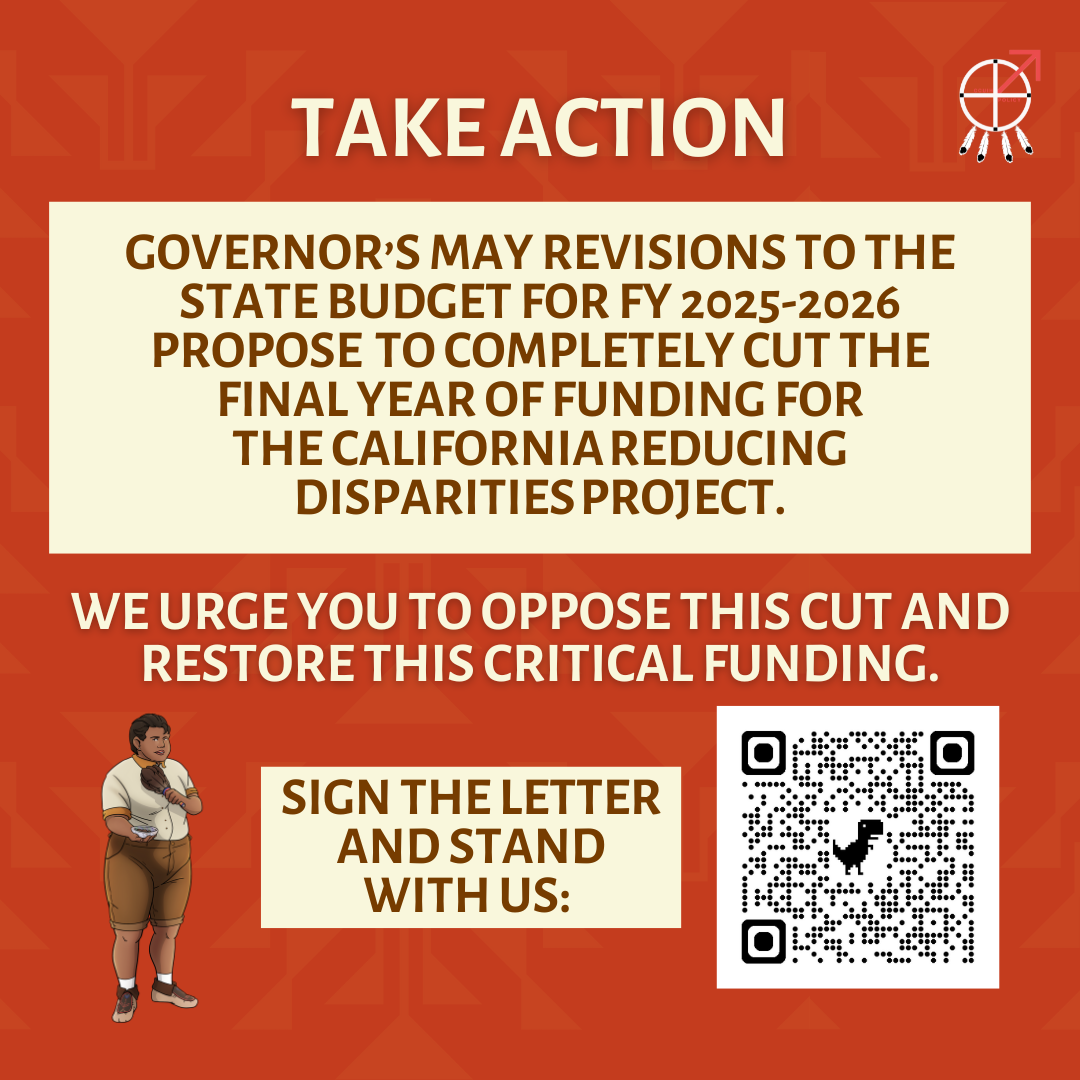
The California Reducing Disparities Project (CRDP)
CCUIH’s Public Statement on the HHS Restructuring and the Creation of the Administration for a Healthy America
